Case Study
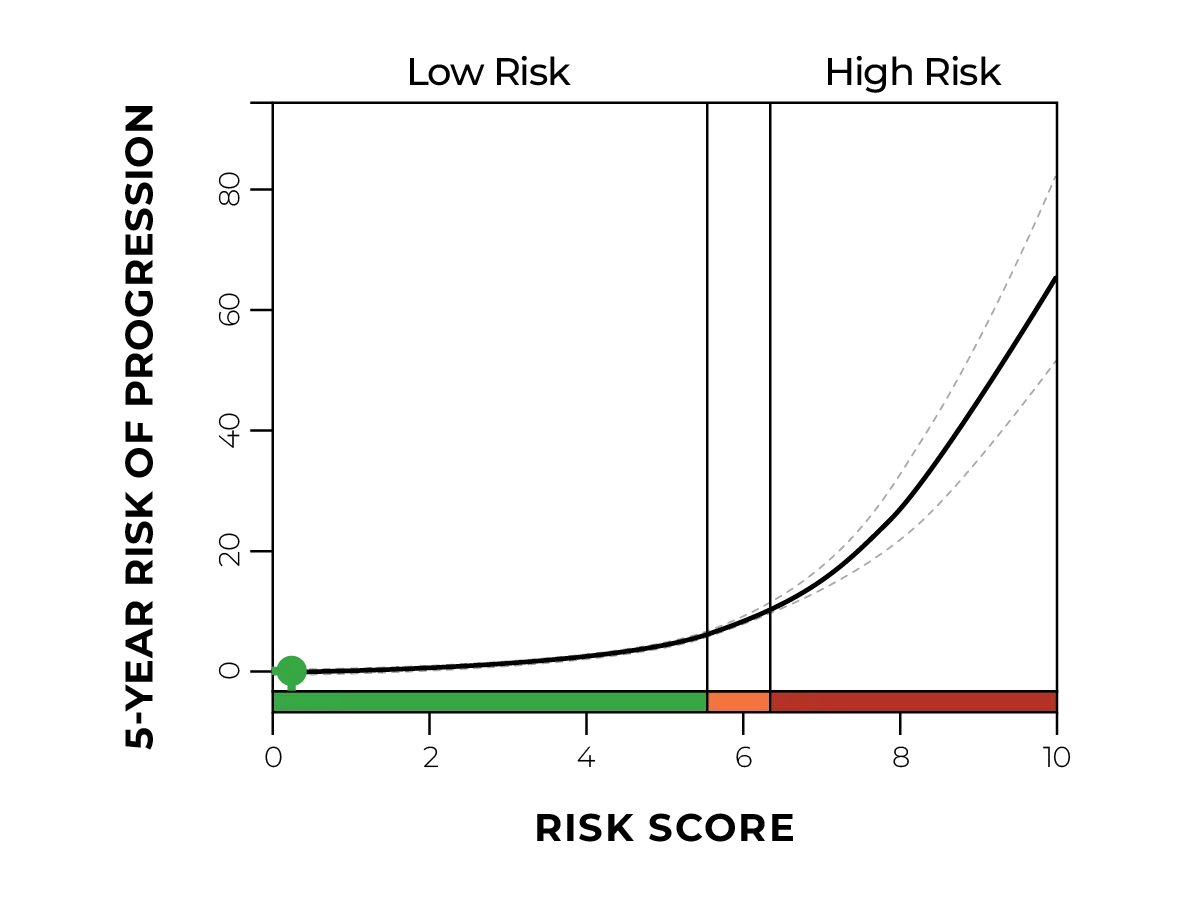
Philip Woodworth, MD, FACS, a foregut surgeon at the Institute for Esophageal and Reflux Surgery, consulted with a patient that was interested in a surgical solution to his long-standing acid reflux. A fundoplication surgery was scheduled, and it included an upper endoscopy that biopsied a 1 cm segment of non-dysplastic Barrett’s esophagus (NDBE).
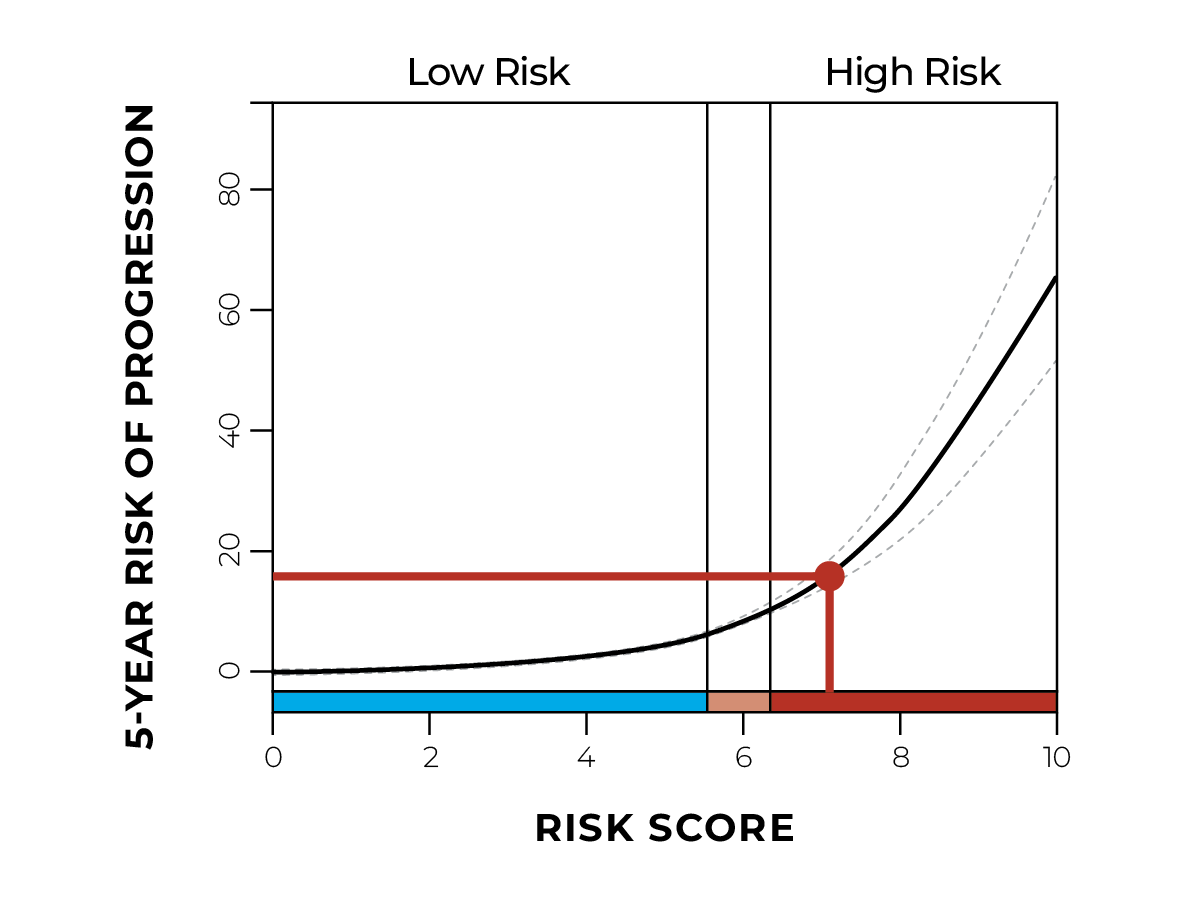
It's standard practice for Dr.Woodworth to order TissueCypher on all NDBE cases, and in this case the results led to a significant change in management.
See the details below to learn how Dr. Woodworth navigated this surprising case.
Case details

- Chronic GERD, long term PPI
- Not especially obese
- No relevant family history
- Non-smoker

- Hiatal hernia














.jpg)